Popular Search Terms
What is knock knees?
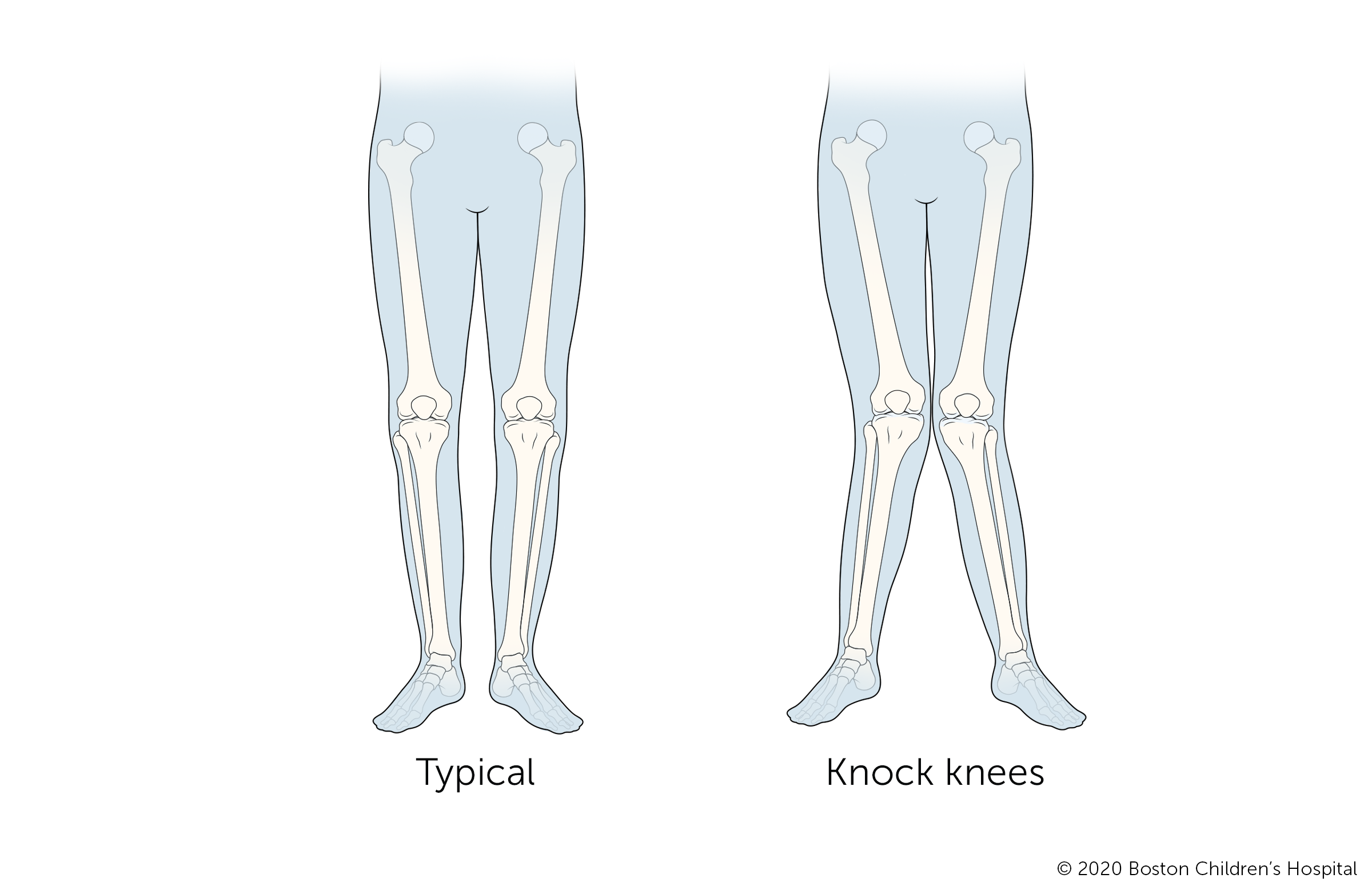
Knock knees (genu valgum) is a condition in which the knees tilt inward while the ankles remain spaced apart. The condition is slightly more common in girls, though boys can develop it too.
Knock knees are usually part of a child’s normal growth and development. Most young children have knock knees to some degree for a period of time, though in some children it is more visible.
In rare cases, knock knees could be a sign of an underlying bone disease, particularly when the condition appears for the first time when a child is 6 or older.
How is knock knees related to a child’s development?
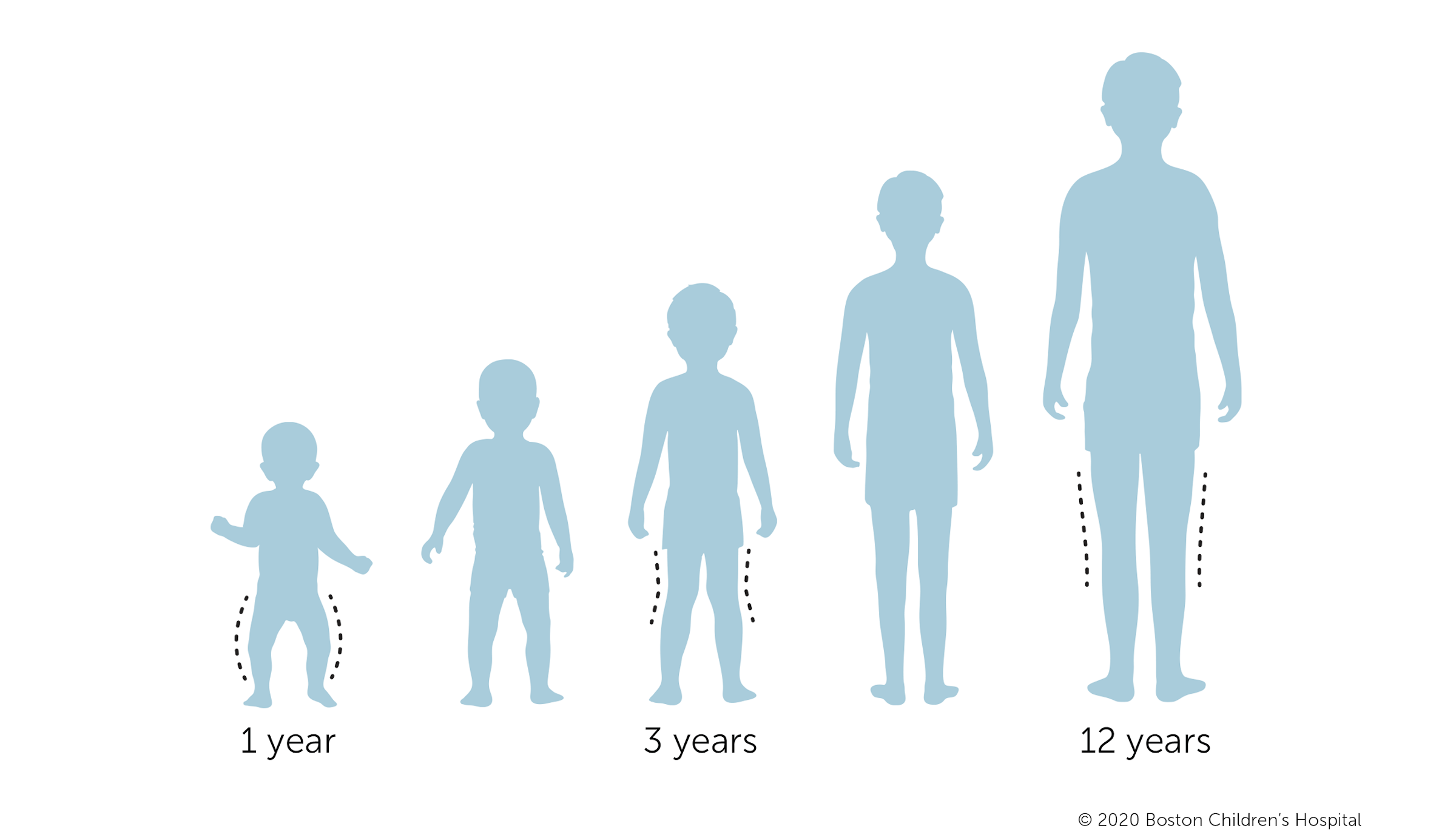
Many children go through stages of bowlegs and knock knees in their early years. As their legs grow and become stronger, the vast majority of children outgrow both bowlegs and knock knees.
- Knock knees in infants: Knock knees are not typical in infants. However, many infants have bowlegs, a condition in which both legs curve outward, up until they are about 24 months old.
- Knock knees in toddlers: Knock knees usually become apparent when a child is 2 to 3 years old. The knees may tilt increasingly inward up until about age 4 or 5.
- Knock knees in young children: Children’s legs usually become aligned by the time they are about 7. Some children continue to have knock knees into adolescence.
When should parents be concerned about knock knees?
If your child has knock knees along with any of the following symptoms, they may have a more serious condition:
- Knock knees that become apparent before age 2 or after age 7
- Knock knees that become worse after age 7
- Asymmetric appearance of the legs
- Limp when walking
- Knee or hip pain
- Short stature (below the fifth percentile)
Symptoms & Causes
What are the symptoms of knock knees?
The symptoms of knock knees are visible when a child stands with their legs straight and toes pointed forward. Symptoms include:
- Symmetric inward angulation of the knees
- Ankles remain apart while the knees are touching
- Unusual walking pattern
- Outward rotated feet
What causes knock knees?
Many children develop knock knees during early childhood. As they begin to walk, an inward tilt at the knees can help children balance. This stance also helps if one or both of their feet roll inward or turn outward.
Less often, knock knees is caused by a more serious disorder:
- Genetic conditions such as skeletal dysplasias or metabolic bone disease such as rickets can cause knock knees.
- Obesity can contribute to knock knees or cause gait abnormalities that resemble knock knees.
- An injury to the growth area of the shinbone (tibia) or thighbone (femur) may result in just one inward-tilting knee.
Diagnosis & Treatments
How are knock knees diagnosed?
Your child’s doctor will look at the position of your child’s legs, knees, and ankles to determine the severity of knock knees. They may also measure the distance between your child’s ankle bones. The condition is considered more severe in children with more distance between their ankles.
Doctors typically look at the following factors to determine if a child younger than 7 has knock knees:
- Weight and body mass index (BMI)
- Height and length
- Position of the knees as the child extends and rotates their legs
- Leg lengths and symmetry
- Walking pattern
If your child is older than 7, or if their legs aren’t the same size and shape on both sides, an X-ray of their legs may help determine if an underlying condition is causing their knock knees.
Doctors do not usually order X-rays for children within the normal age range for knock knees if they have no problem walking, running, or playing, and have typical appearing legs. This avoids exposing the child to unnecessary radiation.
What are the treatment options for knock knees?
In most cases, children with knock knees do not need medical treatment. The most common treatment for children between 2 and 5 years old is close observation. Up to 99 percent of children with knock knees grow out of the condition by the time they turn 7. Children do not need to avoid physical activity, wear braces or special shoes, or do any special exercises.
Non-surgical options for knock knees
If your child has severe, unresolved knock knees, their doctor will first determine if this is part of another underlying condition. If so, treatment will focus on treating the underlying condition. For example, many cases of rickets can be treated with vitamin D and calcium supplementation.
Surgical options for knock knees
In the rare event that natural growth doesn't correct your child's knock knees, their doctor may recommend surgery.
Guided growth surgery
Guided growth surgery corrects knock knees by slowing the growth on the bent side of the bone so the other side can catch up. The surgeon implants small metal devices on the inner side of the growth plates around the knees. The outer side of the knees will continue to grow, causing the legs to grow straighter.
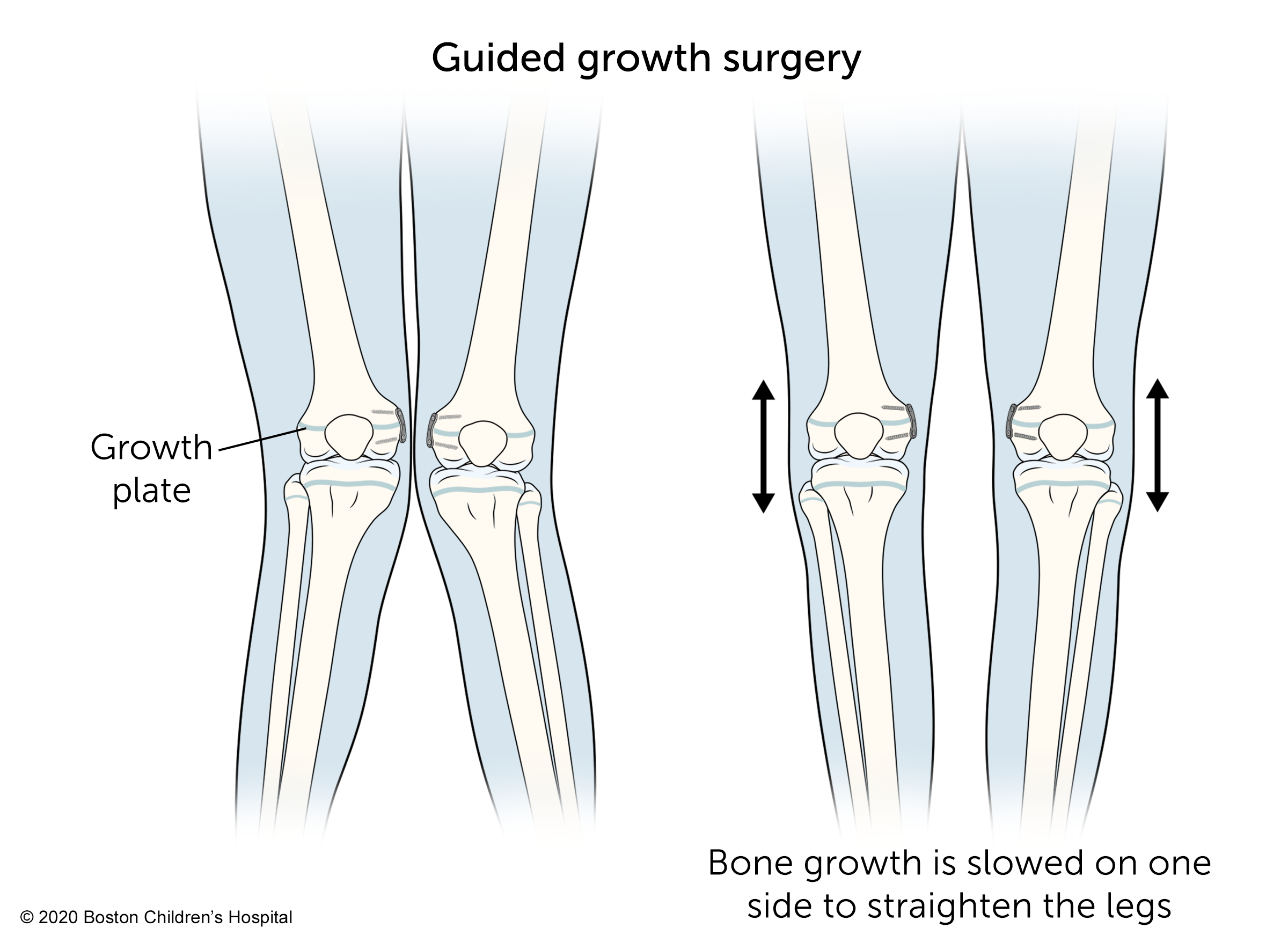
Children usually have guided growth surgery when they're approaching puberty, before their adolescent growth spurt. This is usually around age 11 for girls and 13 for boys.
Guided growth surgery is an outpatient procedure. Children can bear weight on their legs immediately and return to activity within a few weeks after the procedure.
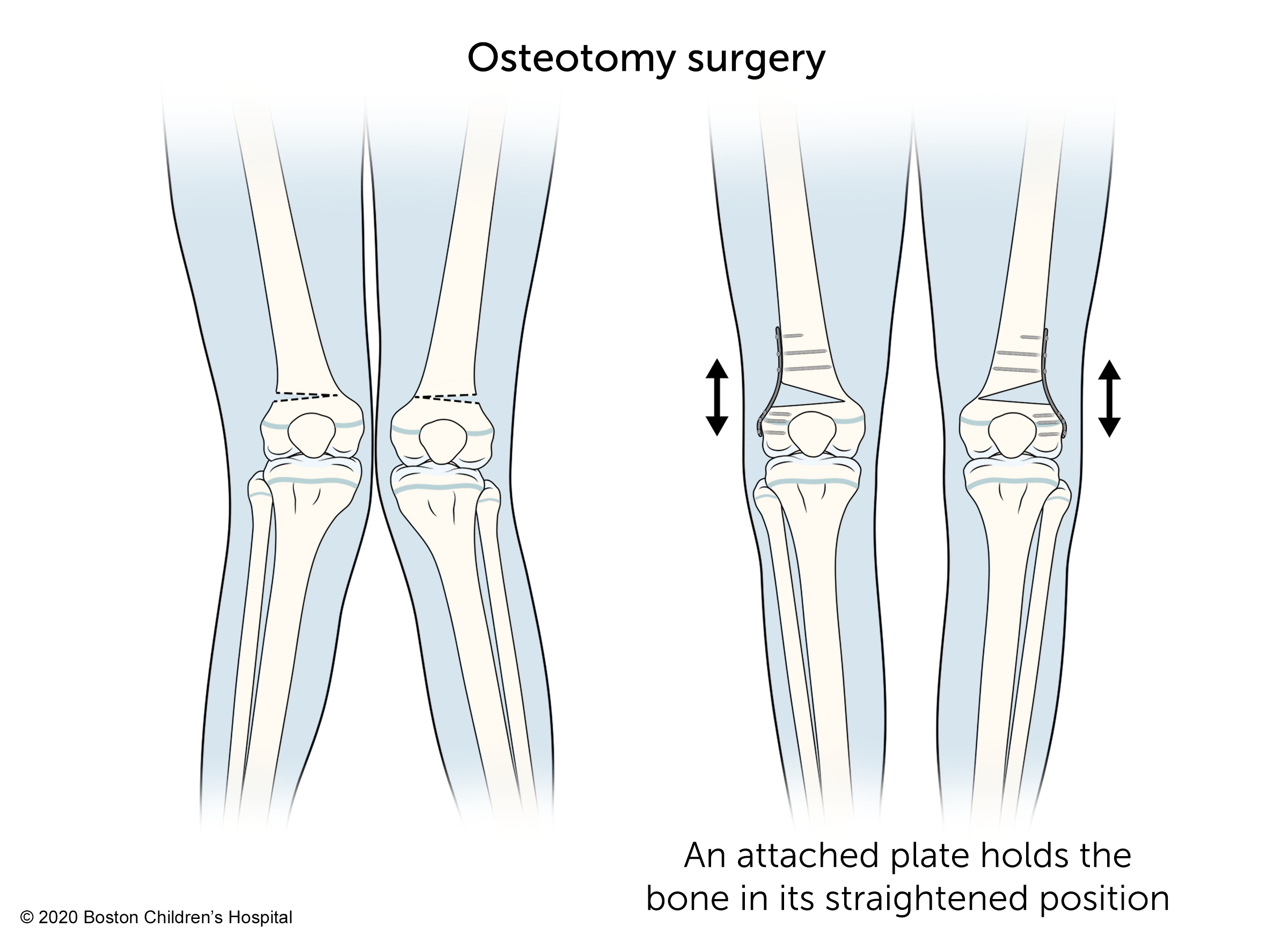
Osteotomy surgery
Osteotomy surgery can correct more severe deformities or knock knees that do not get better on their own by the time a child has finished growing. The goal of this procedure is to straighten the legs by changing the angle of the bones. A surgeon does this by cutting and realigning the bone above or below the knee.
Children typically stay in the hospital for a few days after osteotomy surgery. When they return home, they will need to limit weight-bearing activities and may need to use crutches or a walker for six to eight weeks. Physical therapy will help restore muscle strength. Typically, children can return to full activity, including sports, six months after the procedure.
What is the long-term outlook for children with knock knees?
The vast majority of children with knock knees get better without treatment and have a very positive long-term outlook. For children who have surgery for severe forms of the condition, the outlook is also excellent. The surgical and non-surgical procedures are quite safe and children's bones usually heal faster and more reliably than adults.
Some children with severe knock knees that doesn’t improve or is due to an underlying condition (pathologic valgus), and who do not receive treatment, may over time develop knee pain, meniscal tears, patellar (kneecap) dislocation, or cartilage damage (arthritis).
How we care for knock knees at Boston Children’s Hospital
As a national and international orthopedics referral center, our Orthopedics and Sports Medicine Department has vast experience managing all aspects of knock knees. Our Lower Extremity Program offers comprehensive assessment, diagnosis, and treatment for children and young adults with conditions affecting their lower limbs. We have extensive experience treating disorders of the feet, ankles, knees, legs, and hips. Whether the patient is an infant, child, or adolescent, our goal is to help our patients live full, independent lives.
Practitioners Who Specialize In This Condition (4)

Colyn Watkins, MD
Orthopedic Surgeon, Orthopedics and Sports Medicine Department
Assistant Professor of Orthopedic Surgery, Harvard Medical School


Elspeth Hart, DScPAS, PA-C, MPAS, ATC, LAT
Physician Assistant, The Micheli Center for Sports Injury Prevention a Division of Sports Medicine